
Cardiology Case #22
Primary Author: Dr Alastair Robertson; Co-Authors: Dr Hywel James and David Law
Background:
A 38 year old female is brought into ED by ambulance after being found at home following a suspected intentional overdose around 2 hours previously. Empty packets at the scene suggests she may have ingested valproate, diazepam, zolpidem, and panadeine forte (paracetamol/codeine).
On the arrival of paramedics she was GCS 14, but hypoxic with bilateral crepitations so was placed onto CPAP.
On arrival in ED she was agitated with a deteriorating GCS. Chest revelaed bilateral widespread crepitations. Observations were:
RR 35, sats 95% on CPAP at 100% oxygen, HR 90, BP 160/90, temp 36.5
The patient was too agitated and unstable for much more assessment but rapid POCUS was utilised to assess lungs and subxiphoid cardiac views.
Lung US showed lung-sliding and bilateral B-lines throughout the anterior chest
Subxiphoid view (and ECG) is shown below.
What is your assessment and immediate next steps?
RESUS POCUS:
The focus on this case is the pragmatic use of POCUS in ED. In the unstable or agitated patient investigations and management can be very difficult. Here we can see the value of a rapid POCUS assessment.
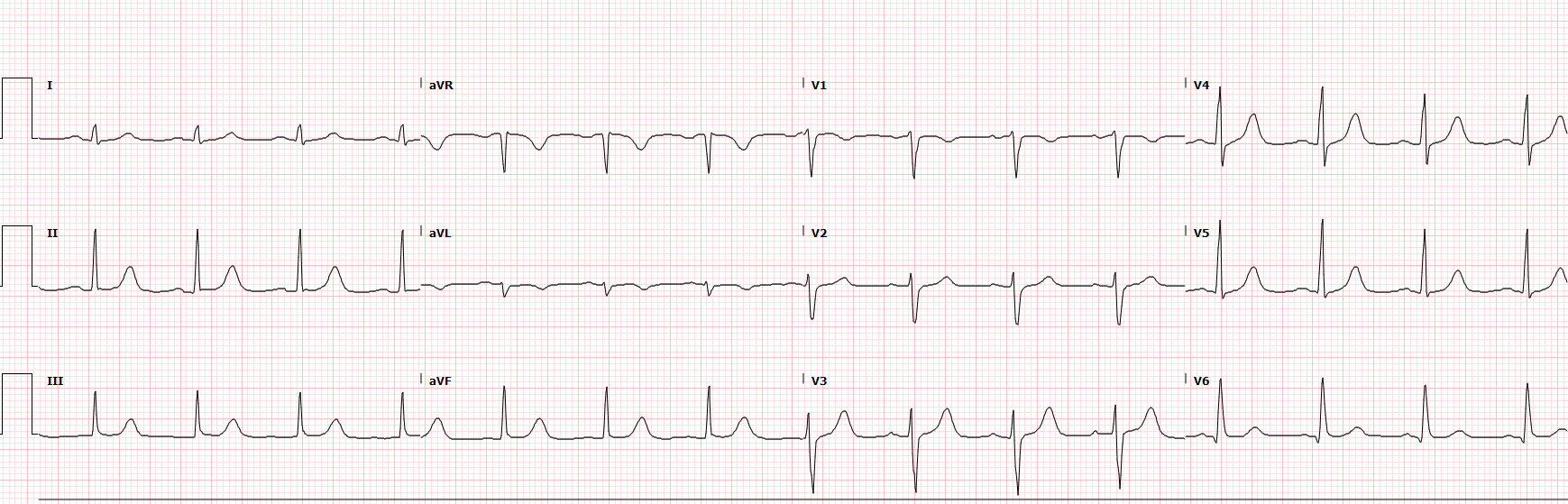
Fortunately we were able to get an ECG but it did not help us, it shows normal sinus rhythm with a normal axis. There is perhaps some very subtle non-specific ST depression and TW inversion laterally (I and aVL). Importantly, in the setting of overdose there is no QRS widening (to suggest sodium-channel blockade), or prolongation of the QT interval.
Lung Ultrasound has confirmed the presence of bilateral B-lines (images not shown) which excludes pneumothorax, as well as suggesting a systemic pathology such as:
cardiogenic pulmonary oedema, or non-cardiogenic (e.g. ARDS)
bilateral inflammatory process e.g. viral pneumonitis
other fluid overload states (renal or hepatic failure)
chronic conditions such as pulmonary fibrosis
Massive aspiration or pneumonia is possible, but symmetrical findings in the anterior chest are more suggestive of APO or pneumonitis (in the absence of known fibrotic lung disease).
Subcostal 4-chamber view shows at least moderate impairment of LV function. Interestingly there is contractility towards the apex (more on this later). Importantly, we can see there is no significant pericardial effusion, and the RV is not dilated.
Therefore, in a matter of seconds, we have identified likely acute LV failure with pulmonary oedema, as well as excluding pericardial effusion, pneumothorax, or acute RV failure.
This patient was not behaving like a typical drug overdose.
Case Progress:
The patient was optimised on BiPAP and then a delayed sequence intubation on VAPOX (ventilator-assisted pre-oxygenation) was performed due to simultaneous deteriorating respiratory status and GCS.
Further collateral revealed that her ingestion was predominantly sedatives (benzodiazepines and zolpidem). Valproate ingestion was most likely modest (around 200mg/kg). Of note she was also prescribed MR Venlafaxine. She had also had a cough for several weeks, and had completed 2 course of antibiotics in the community.
At this point the differential was wide, and included toxicological cardiac toxicity, viral myocarditis, hypoxia or aspiration from overdose, cardiomyopathy due to other cause (ischaemia, arrhythmia, stress, or sepsis).
Chest XR (shown below) confirmed dense bilateral infiltrates more in keeping with pulmonary oedema/ARDS rather than infection or aspiration.
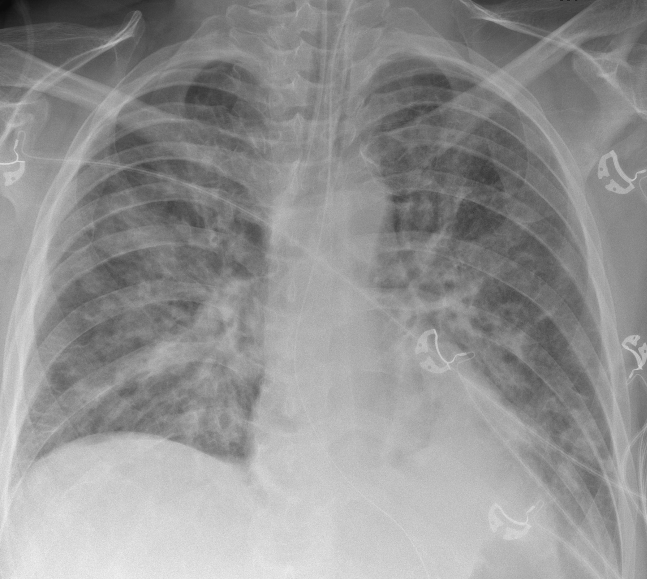
CXR showing appropriately placed ETT and NGT, with bilateral pulmonary infiltrates.
The patient remained hypertensive at 170/90 despite adequate sedation so a GTN infusion was started.
Ventilation focussed on ensuring oxygenation with adequate PEEP.
Activated charcoal was given via NGT.
Cardiac POCUS
Further cardiac ultrasound was employed in an attempt to elucidate the cause of the LV impairment. Intubated patients are often difficult to scan due to positioning and positive pressure ventilation but the key is to acquire adequate rather than perfect pictures.
See the clips below. What do you think of the LV function?
Basic POCUS: the low PLAX
The view above is a low parasternal view rather than a “true” PLAX as the LV is angled upwards. This is in incredibly useful view in ED in patients who do not have a good parasternal window. Place the probe in the low left parasternal region (often around 5th or 6th ICS) and angle back up towards the heart. The advantage is that we get most the information of a PLAX view but we can also visualise the apex.
Here we can see that there is LV impairment. The LV base and mid-cavity are contracting very poorly. We can see that the LV apex is working however, which would have been missed had we not visualised the apex.
The important point to note is that the apex is contracting well both anteriorly (distal anterior septum) and posteriorly. Likewise, the LV impairment is symmetrical involving both the anterior and posterior walls of the LV base & mid-cavity. This is segmental impairment, but not in a way which would fit a vascular territory.
LV impairment was thought to be moderate-to-severe (EF estimated around 30%). Whilst methods such as fractional shortening, or EPSS (see Case 19 - LV function) they will underestimate the EF in cases such as this where the apex is hyperdynamic to compensate for basal LV impairment.
Using a systematic approach, this low PLAX confirms there is no large pericardial effusion (probably trivial effusion), the mitral valve appears grossly normal, and the RV:aorta:LA sizes all appear appropriate.
Now review the two PSAX clips below
Intermediate POCUS: putting it together
Remaining in the parasternal window (now SAX) we can see the top clip is in the region of the LV base/mid-cavity. Here we confirm that there is global impairment of all the vascular territories in the PSAX.
In contrast, the bottom clip of the LV apex shows a symmetrical normal or hyper-dynamic apex. Additionally you can see the lung B-lines coming across the screen with respiration. Healthy lungs would create a dark lung shadow, but the bright white B-lines signify “interstitial syndrome”, pulmonary oedema in this case
So what is going on here? Symmetrical LV basal impairment with a compensatory hyperdynamic apex does not fit a particular vascular territory. Nor is it consistent with a viral myocarditis, and is the opposite pattern of a typical takotsubo cardiomyopathy.
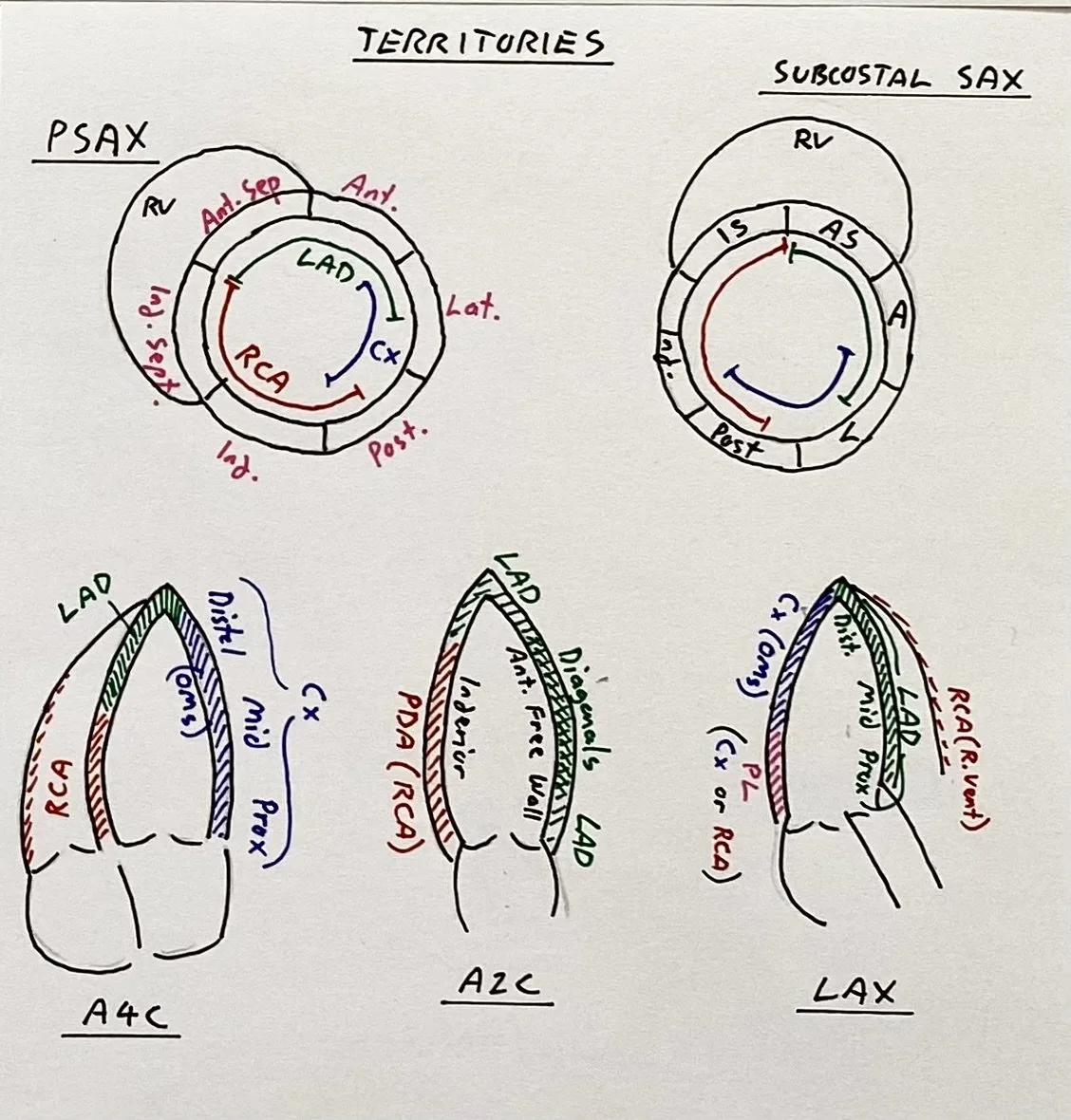
Remind yourself of the typical vascular LV territories seen on echo.
Case Progress:
The patient was managed supportively, but there were some ventilation issues with high pressures and also unexplained hypoxia which will be discussed below. She had a rising lactate but remained haemodynamically stable despite the cardiomyopathy.
Valproate levels were not significantly elevated. Paracetamol level, salicylate level, and osmolar gap were all normal. The echo findings raised suspicion for an atypical or ‘reverse’ takotsubo cardiomyopathy, which has been descrbied in venlafaxine overdose (venlafaxine can also be incredibly cardio-toxic in large overdose).
She stabilised in ICU and after a formal echo the working diagnosis was an atypical takotsubo cardiomyopathy which improved rapidly over the next 24 hours. Unfortunately further details on exactly what medications she had taken were not forthcoming on extubation.
FOCUS on: Atypical Takotsubo
We have covered Takotsubo previously, click here to review Case 18.
Classic or ‘Apical’ Takotsubo is the most common (around 80% of cases), and involves symmetrical apical hypokinesis extending past a single vascular territory. The LV base is often hyperdynamic to compensate which can cause complications such as dynamic LVOTO. About a third of cases will also have apical RV impairment. Classic Takotsubo can be difficult to differentiate from LAD ischaemia as the LV apex is predominantly supplied by the LAD so is a diagnosis of exclusion after angiogram.
Atypical Takotsubo accounts for about 20% of cases and there are several types. Aetiology is thought to be due to individual distribution of adrenoceptors around the myocardium which are overwhelmed by a sympathetic surge.
Reverse or ‘Basal’ Takotsubo as seen in this case accounts for only 2% of cases. It is more common in younger patients, often with some kind of organic or medical stress rather than emotional stress. Risk of LVOTO is minimal due to its basal location but it can cause mitral regurgitation due to basal hypokinesia, remodelling and papillary muscle involvement. It is easier to prove hypokinesis spreading past vascular territiroeis in the basal regions due to the anterior, inferior, and lateral walls all having a different blood supply.
Mid-Cavity Takotsubo as seen in Case 18 accounts for about 15% of cases, and demonstrates symmetrical hypokcinesis of the LV mid-segments creating a ‘reverse hourglass’ shape. This can create a mid-cavity pressure gradient and complications include LV thrombus, or wall rupture due to increased stresses.
Focal Takotsubo involves a discrete part of the LV, often the anterolateral wall, which can make it indistinguishable from ischaemia without an angiogram.
Atypical patterns of Takotsubo can be challenging as they rarely occur, and will often lack the classic ECG changes of apical Takotsubo. Furthermore they are more likely to occur in younger patients with acute medical, rather than emotional, stresses which makes it important to exclude a direct complication of a medical condition causing cardiomyopathy.
In this case the diagnosis is still unclear. It is possible that a combination of drug overdose and/or recent chest infection had triggered the Takotusbo cardiomyopathy. The patient had access to venlafaxine but it is unclear if she had taken any.
Additional case related pearls:
Venlafaxine is an SNRI anti-depressant which can be toxic in overdose. Toxicity is usually seen as a delayed onset serotinergic toxicity (tachycardia, hyperthermia, clonus, sweating/agitation) due to SRI effect. Venlafaxine also has sodium-channel blockade effect which can cause seizures and ventricular dysrhythmias. At higher doses NRI effect is enhanced leading to catecholaminergic surge which is hypothesised to contribute to the profound cardiogenic shock which can be seen. This patient did not have any clear serotonergic or sodium-channel blockade syndromes. It is possible that a less extreme manifestation of this could be a stress cardiomyopathy from inhibition of noradrenaline reuptake and both typical and atypical (basal) takotsubo-like syndromes have been described in the literature, which are commonly quicker to resolve as the drug effect wears off.
It is unclear if this patient took excess venlafaxine but she had access to it.
Valproate, on the other hand, is a mood-stabiliser and anti-epileptic drug which works by inhibiting voltage-gated sodium channels leading to increased GABA. At the reported dose in this case (around 200mg/kg) it would be expected to produce only mild CNS depression, but at higher doses (>500-1000mg/kg) it can cause profound coma, metabolic acidosis and multi-organ failure, ammonaemia causing cerebral oedema, and hypocalcaemia/hypoglycaemia, and hypernatraemia.
It does not have direct cardio-toxic effects and management for large ingestions focusses on airway support for likely coma, decontamination (charcoal and whole-bowel irrigation), enhanced elimination (dialysis), adjuncts (such as meropenem or carnitine) to decrease toxic metabolisation, and supportive care of acidosis and electrolytes (in particular managing hypernatraemia).
Given severe LV basal hypokcinesis always assess for the amount of MR. In the clip below we can see this patient had only mild MR.