
Cardiology Case #20
Primary Author: Dr Alastair Robertson; Co-Authors: Dr Hywel James and David Law
Background:
A man in his 40s presents to ED with breathlessness. He has felt lethargic and tired for the last month, but has noticed worsening dyspnoea, orthopnoea, and leg swelling associated with a worsening cough over the last 5 days.
He has no other previous medical history other than obesity. He denies chest pain or haemoptysis. He does not take any regular medications. Non-smoker and only moderate alcohol intake.
His observations are: RR 23, Sats 94% on air, HR 98, BP 194/90, temp 37.6.
Chest XR and ECG are shown below.
-
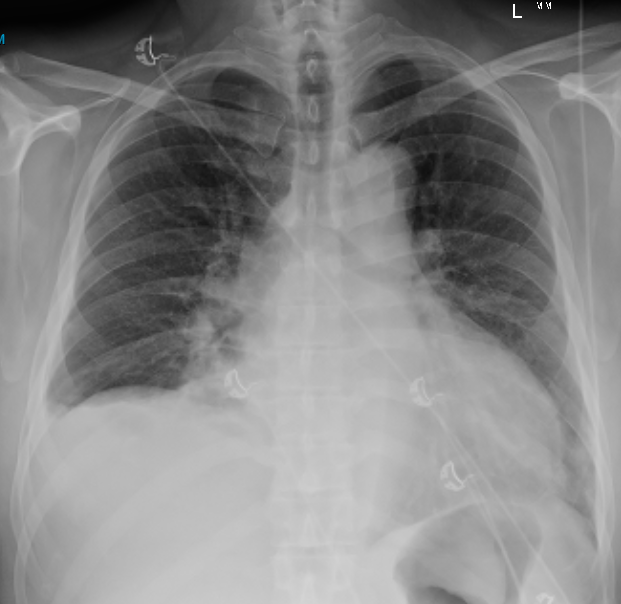
CXR shows:
right mid zone opacification obscuring the right heart border, this could be infective or congestion.
There is a right pleural effusion, and upper lobe diversion/infiltrates suggesting some pulmonary oedema
Marked cardiomegaly
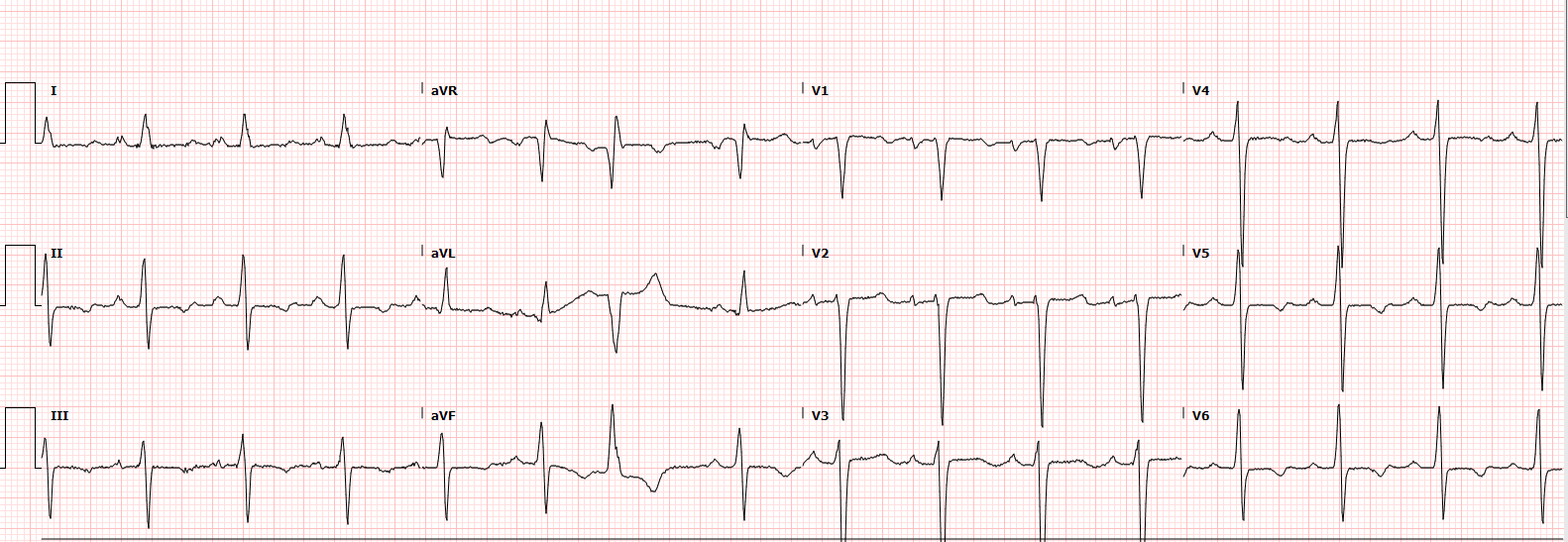
ECG shows:
sinus rhythm at a rate of around 96/min with a PVC.
Left axis deviation with a LAFB
Poor R-wave progression in precordial leads, and T-wave inversion inferno-laterally but no specific ST changes.
Cardiac POCUS:
This is a young patient presenting with possible features of cardiac failure so POCUS is useful to assess cardiac function. If cardiac failure is present then we want to know why, particularly given his elevated blood pressure. Understanding the aetiology of the problem is key to guiding resuscitation and management.
Below are the Parastenal Long Axis (PLAX), and an Apical 4-chamber views (A4C).
What do you think is happening?
How would you describe the LV function?
Basic POCUS: global assessment
The information from the PLAX clip (top) is immediately significant.
There is no pericardial effusion
The LV function is very poor. The LV is also significantly dilated. This is severe LV impairment (severe is EF <30%). See Case 19 for a review on LV function but the EF here was measured at 20%.
Also note the LV wall thickening, which shows LV hypertrophy.
Looking at the RV:Ao:LA we can see that the RV looks normal, but the Aorta, and the Left Atrium both appear dilated. In particular the Aorta is very prominent.
The A4C (bottom) clip confirms that we have a very dilated LV with Severe global LV Impairment. If you look towards the crux of the heart, you can see the aortic root coming into the clip. When trying to get a 4-chamber view it is often difficult to get the aorta out of shot if it is dilated.
So in summary, we have severe LV dilation, and severe LV impairment. We also have a very prominent aorta and left atrial dilation. This patient is in significant heart failure, but why is his aorta dilated, and what is the underlying cause?
Steps beyond Basic POCUS: The Aorta
Measuring the aortic root, and the ascending aorta is an important skill in echo. Pathologies which can be picked up include aortic dissection, thoracic aortic aneurysm, hypertensive heart disease, aortic regurgitation, aortic root aneurysm.
Measure the aortic root at the widest point (sinuses of valsalva) on the PLAX axis. The aorta should then narrow to the sinotubular junction. The ascending aorta is measured 1-2cm distal to this, ideally where it runs parallel. Both Aortic root and ascending aorta are measured at end-diastole ideally.
Tips:
From PLAX (3rd or 4th IC space, left parasternal) move up a rib-space gives better images of the ascending aorta (and sometimes the root)
Measure from ‘leading edge to leading edge’ and ensure you measure perpendicular across the aorta.
Rotate the probe slightly to open the aortic root as much as possible as you can see on the drawing below (SAX view) the measurement of the widest point is not actually through the centre of the valve.
The aortic valve is hinged up to its insertion at the sinotubular junction (STJ - where the root narrows in), which can also be measured.
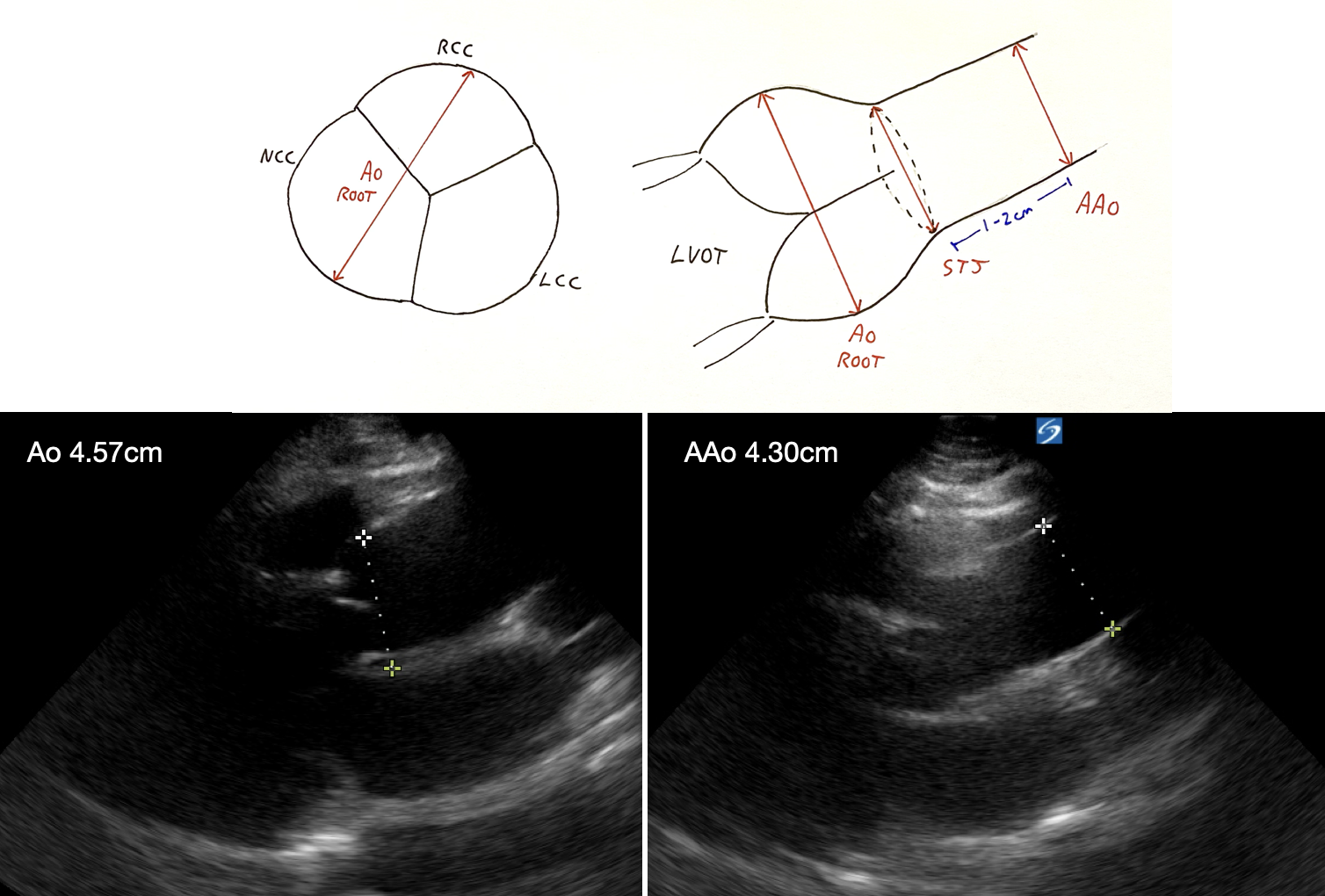
In this patient you can see the Aortic Root (abbreviated to Ao, a.k.a Sinus of Valsalva) was 4.57cm and the Ascending Aorta (or AAo, a.k.a Tubular portion of proximal ascending aorta) was 4.30cm.
As a general rule, normal measurements are < 40mm for the aortic root, and < 35-38mm for the ascending aorta, however these are usually indexed to sex and BSA so the upper limit of normal can vary and will be lower than these values in some patients. Generally, the diameter of aorta should become smaller from ascending (<38mm), through the arch (<35mm), to descending (<30mm).
So this patient has a dilated aortic root, as well as a dilated ascending aorta. You may also note that we have lost the usual ‘pinching in’ at the sinotubular junction as both the root and the aorta itself are dilated.
Pathologies to consider when you identify a dilated aortic root, or ascending aorta include:
Systemic hypertension/atherosclerosis
Aortic valve disease (stenosis/regurgitation)
Acute aortic dissection or intra-mural haematoma
Congenital (bicuspid aortic valve) or connective tissue disease (Marfan’s, Ehlers-Danlos Syndrome, Loeys-Dietz Syndrome)
Inflammatory (Giant Cell Arteritis/Takayasu’s) or Infectious (Syphilitic Aortitis, Aortic Root abscess from IE)
Previous surgical intervention, or congenital cardiac disease.
Intermediate POCUS:
This patient has severe LV impairment and assessing the valves is important. A dilated aorta in particular is concerning for aortic valve pathology. We also want to assess the mitral valve and pulmonary pressures. Identifying severe valvular pathology is crucial as it will often significantly alter resuscitation and management, particularly with regards to BP and HR control. Below is a:
PSAX at the LV mid-cavity (top)
PLAX of the aortic valve (colour doppler)
A4C of the LV (with colour doppler)
POCUS interpretation:
PSAX (TOP):
We can see here the poor LV function in short-axis. What is also appreciable is LV wall thickening, suggestive of significant hypertrophy.
PLAX (MIDDLE):
Here you can see an Aortic Regurgitation jet, which is a diastolic jet. It is directed posteriorly towards the bottom (posterior wall) of the LV. Whilst the jet does not look particularly broad, these kind of posteriorly directed jets (think of them like eccentric MR jets) can be more severe than they initially appear.
A4C (BOTTOM):
This is not a true A4C as you cannot see the mitral valve. It is an image from the A4C position but the probe has been tilted down to catch the posterior part of the ventricle and foreshortened slightly. As the aorta is a superior structure, flow from AR flows round the posterior part of the ventricle, and this this view is to tries and catch it. Here you can see an impressive regurgitation jet flowing posteriorly round to the lateral wall and all the way up towards the apex.
This combination of hypertrophy, with a broad extensive regurgitant jet is concerning for SEVERE AORTIC REGURGITATION.
Of note, this patient had only mild-to-moderate function mitral regurgitation, and no aortic stenosis.
So likely Severe AR which is important to pick up as we will see below.
FOCUS on: Severe Aortic Regurgitation
Intermediate/Advanced POCUS
Why do we need to know?
Some AR is not uncommon. Mild or Moderate AR are generally haemodynamically stable lesions which don’t usually need addressing in ED as they don’t change our management or need specific resuscitation strategies.
Severe AR is a different beast with significant haemodynamic complications to consider.
Will it change management?
Yes, Severe AR often dictates specific HR and BP parameters to avoid haemodynamic compromise, and also needs consideration as is incompatible with some mechanical supports.
OK, how do I diagnose it?
Diagnosing Severe AR can be tricky, and is not always easy to pick up from the colour doppler or valve itself. One way to approach this is to look carefully at the Left Ventricle. Severe AR is the lesion that puts the most stress on the LV, as it causes LV pressure afterload, as well as LV volume overload. The state of the LV tells you about the haemodynamic severity of the regurgitation.
If you see what looks like Aortic Regurgitation on colour doppler start looking for:
LV Findings suggesting Severe AR:
A dilated LV is common (diameter >5cm) from volume overload. As Severe AR progresses, the LV may lose it’s usual ellipsoid shape and become more spherical.
LV hypertrophy from wall/volume stress. Looks for thickened LV walls. In AR the myocytes enlarge to cause ‘eccentric’ hypertrophy which means increased LV mass due to both pressure and volume overload.
The LV is usually hyper-dynamic to compensate for the lost forward volume (similar to Severe MR). The difference in AR is the regurgitant blood is causing LV volume overload. As the LV progressively fails the stroke volume will drop, and an impaired LV with worsening dilation/volume overload is a sign of decompensation and impending haemodynamic collapse.
You may see ‘fluttering’ of the anterior mitral valve leaflet (on 2D or M-mode) from the AR jet, or even premature mitral valve closure as the diastolic LV pressures rapidly rise and overcomes left atrial pressure in diastole.
Doppler Findings suggesting Severe AR:
A broad colour doppler jet occupying >65% of the LVOT diameter suggests Severe AR, best picked up in the A4C but also the PLAX.
A regurgitant jet wrapping around the LV all the way up to the apex (on A4C, tilt posteriorly, towards spine, to pick up the flow)
A regurgitant fraction (i.e. amount the stroke volume which flows back into the LV) of >50%, or absolute volume of >60mL is Severe AR. Whilst difficult to measure this, given that a normal stroke volume in a stable patient is around 70mL we can deduce that if a stable patient has a calculated SV of >120ml (regurgitant volume must be around 60mL) they likely have Severe AR. This becomes difficult in patients with severe LV dysfunction or hypotension.
Aortic Findings suggesting Severe AR:
Aortic doppler is important in identifying Severe AR. Aortic dilation is common but looks at the flows in the aorta.
Significant reverse flows in descending thoracic aorta suggest Severe AR.
Reverse colour flow during diastole in the Abdominal Aorta, or pan-diastolic reverse flow in Abdominal Aorta Doppler
Clinical Findings suggesting AR:
Look for a wide pulse-pressure, pan-diastolic murmur at left sternal edge (worse sitting forward), and a collapsing or ‘waterhammer pulse’. Displaced apex beat may suggest LVH.
Acute vs Chronic Severe AR
LV hypertrophy and dilation are found in chronic AR. Acute AR will usually cause a hyper-dynamic LV as the ventricle has not had time to remodel.
Likewise, diastolic reverse flow in the abdominal aorta more commonly seen with acute AR.
Acute AR causes a high-density regurgitation jet on CW doppler (through aortic valve on A5C) with a peak-to-end time of <250ms. This finding is less reliable in Chronic AR.
In Summary
Detecting Severe AR can be tricky. Firstly, use your basic skills to look at the LV for concerning features. Then put this together with your colour doppler, and aortic doppler tracings to guide suspicion for Severe AR.
This patient had LV findings suggestive of Severe AR, and a broad large colour jet. He also had significant reverse flows in the thoracic aorta.
Below you can see a SAX view of his aortic valve (centrally located). You can see a tri-leaflet valve with a central triangular gap in diastole (called a coaptation defect) which is the hole which is causing the regurgitation. The bottom picture shows an example of PW doppler in the descending thoracic aorta (not this patient). Systole is shown in red, and green shows continues reverse flow through the entire of diastole (so called ‘holo-diastolic’) signifying Severe AR.
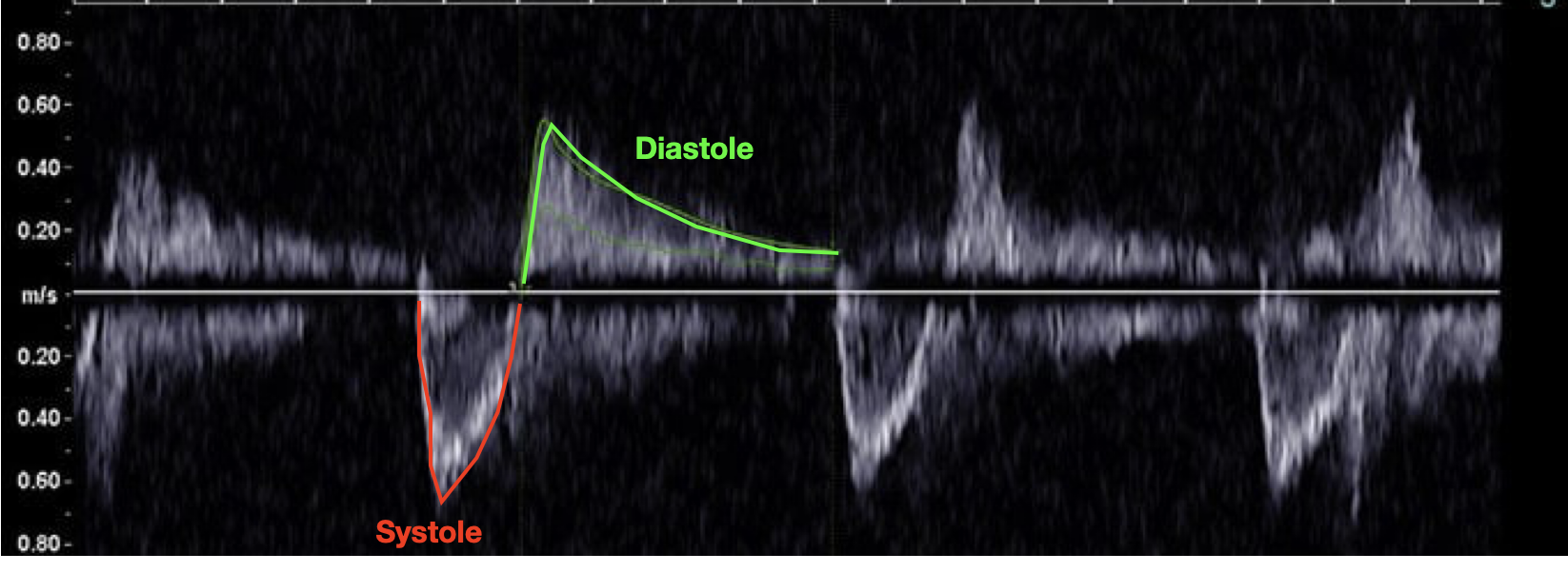
Bottom image from Arunachalam et al. (PMID 33117948)
Case Progress:
The patient was admitted under Cardiology and diagnosed with a concurrent RSV infection, but fortunately remained reasonable stable. He was diuresed with a focus on afterload reduction and fluid status optimisation. He was diuresed by over 12L to become euvolaemic. Given the AR, beta-blockers were withheld.
Further transthoracic echo and TOE showed a aortic valve with a large coaptation defect causing Severe Aortic Regurgitation. The cause of this was likely chronic hypertension causing aortic root/ascending aorta dilation which had effaced the sinotubular junction (the distal aortic valve attachment point), and as this had dilated it pulled the leaflets apart causing the AR.
Once euvolaemic he was worked up for an aortic valve replacement, which included a CT Aorta, coronary angiogram, right heart catheterisation, lung function tests, and dental clearance (see Case # 17 for more details on valve replacement workup).
FOCUS on Severe AR: Causes & ED Management
Causes of Chronic Aortic Regurgitation:
Aortic root dilation - usually hypertension or connective tissue disease
Chronic aortic dissection or aneurysm
Rheumatic heart disease (most commonly involved valve after the mitral)
Bicuspid Aortic Valve
Degenerative Valve Disease
Dilated LV/Cardiomyopathy (altering LVOT architecture)
Causes of Acute Aortic Regurgitation:
Infective endocarditits ± valve rupture
Acute aortic dissection (Type A)
Trauma (Blunt Aortic Injury)
Prosthetic aortic valve failure
Management principles for Acute AR in the ED:
In the unstable patient these lesions are incredibly volume-sensitive.
Volume overload/hypertension can precipitate haemodynamic collapse.
These patients are highly sensitive to afterload
i) Target the lowest acceptable blood pressure
this will minimise regurgitation and decrease LV overload
the caveat is that a diastolic BP of at least 50-60mmHg is probably required to allow sufficient coronary artery perfusion.
LV function should be hyperdynamic (tachycardia and reduced diastolic time is protective)
If Forrester II (‘warm and wet’) then:
consider afterload reduction with e.g. GTN or Clevidipine
consider preload reduction with e.g. GTN if concurrent pulmonary congestion
If Forrester IV (‘cold and wet’) then:
these patients are in a bad place, likely with a failing LV
defend the MAP to allow diastolic filling, use echo to find the balance between inotropes and vasopressors to provide the lowest acceptable BP.
If inotropy is required, consider Adrenaline, Dobutamine, or even Milrinone
Primary vasopressors such as Noradrenaline, Metarminol, or even Phenylephrine may be useful to increase diastolic BP without increasing myocardial oxygen demand if LV function is sufficient.
There is no good evidence one particular agent is superior to any others.
ii) NIV can be useful for respiratory distress/pulmonary oedema
CPAP, or BiPAP with a small pressure support will help decrease LV preload and afterload.
HFNP is another option to provide a small amount of PEEP.
iii) Avoid Arrythmia
Target a heart rate of 90-120 to optimise cardiac output - tachycardia decreases diastolic (regurgitant) time.
Avoid slowing the HR below this with beta-blockers
Treat AF with RVR aggressively as loss of atrial kick is often poorly tolerated
consider Amiodarone, DCCV, or digoxin if needed. Avoid beta-blockers.
In Aortic Dissection with acute AR exercise extreme caution with beta-blockers, tachycardia may have to be tolerated in this instance despite the usual endpoint being to lower HR.
iv) Consider Mechanical Supports
the failing patient may need mechanical support as a bridge, but this is tricky in AR as supporting aortic pressures will feed back to cause LV overload.
importantly, IABP is contra-indicated in Severe AR
Impella, and VA ECMO are relatively contra-indicated - seek specialist advice and consider alternatives such as Left Atrial VA-ECMO.
v) Early Surgical Referral
for consideration of surgical intervention